A SCOPING REVIEW“Add-ons” to IVF
By Lyka Mochizuki, MSc, who was a research associate at the Center for Human Reproduction (CHR) in New York City until 2024 and now is a Visiting Scientist. She introduced conflict resolution into controversial issues in the reproductive medicine literature, starting with preimplantation genetic testing for aneuploidy (JARG 2020;37:677-687), and can be contacted through the editorial office of The Reproductive Times.
Briefing: A recently published review article on “add-ons” to IVF in the medical journal Human Reproduction was the impetus for Lyka Mochizuki, MSc., a former research associate and current Visiting Scientist at the Center for Human Reproduction in New York City, to go somewhat beyond the scope of our usual literature review of a single paper and offer a Scoping Review of the subject with what we believe are some important new insights. We believe you will agree and, therefore, are featuring her comments here as an independent article.
In vitro fertilization (IVF) has been a groundbreaking advancement in reproductive medicine, offering hope to individuals and couples facing infertility. However, the emergence of IVF “add-ons” — optional treatments and procedures marketed as success rate enhancer (1) — has sparked significant debate within the medical community. Many of these add-ons lack sufficient scientific evidence to prove their efficacy, leading to ethical concerns, increased financial burden on patients, and professional disagreements among fertility specialists.
IVF “add-ons” include treatments such as embryo glue, assisted hatching, preimplantation genetic testing for aneuploidy (PGT-A) in younger patients, immunological therapies, endometrial scratching and many more tests, instrumentations, and procedures. While all of these interventions are often marketed as ways to improve implantation and pregnancy rates, scientific studies have often failed to support their effectiveness.
They, therefore, often may lack high-quality evidence as Maheshwari et al., for example, already suggested as early as 2016 for routine blastocyst-stage embryo transfer (2) and in 2022 for routine delayed frozen in comparison to fresh blastocyst stage embryo transfers (3), both “add-ons” to IVF, the CHR identified as likely leading contributors to declining live birth rates in IVF in the U.S since 2010 (an observation further discussed and referenced below). These “add-ons” are lacking robust randomized controlled trials (RCTs) demonstrating their efficacy.
The UK’s Human Fertilisation and Embryology Authority (HFEA), therefore, has categorized most add-ons as “red” or “amber” on their traffic-light rating system, meaning there is no or conflicting evidence supporting their benefits (4). Studies on endometrial scratching, for example, have not shown
consistent improvements in implantation rates (5).
“Add-ons” may also contribute to a placebo effects and other psychological influences, as many patients undergoing IVF feel pressured to try anything that might improve their chances of success, leading to emotional and psychological bias in evaluating these treatments. Perceived benefit may, therefore, be due to placebo effects rather than actual physiological improvements (6).
“Add-ons” also may cause financial and ethical concerns: They unquestionably increase the costs of treatment, placing additional financial strain on patients without clear benefits. Professional bodies like the American Society for Reproductive Medicine (ASRM) and the European Society of Human Reproduction and Embryology (ESHRE), therefore, discourage the routine use of unproven “add-ons,” citing concerns about misleading claims and lack of transparency.
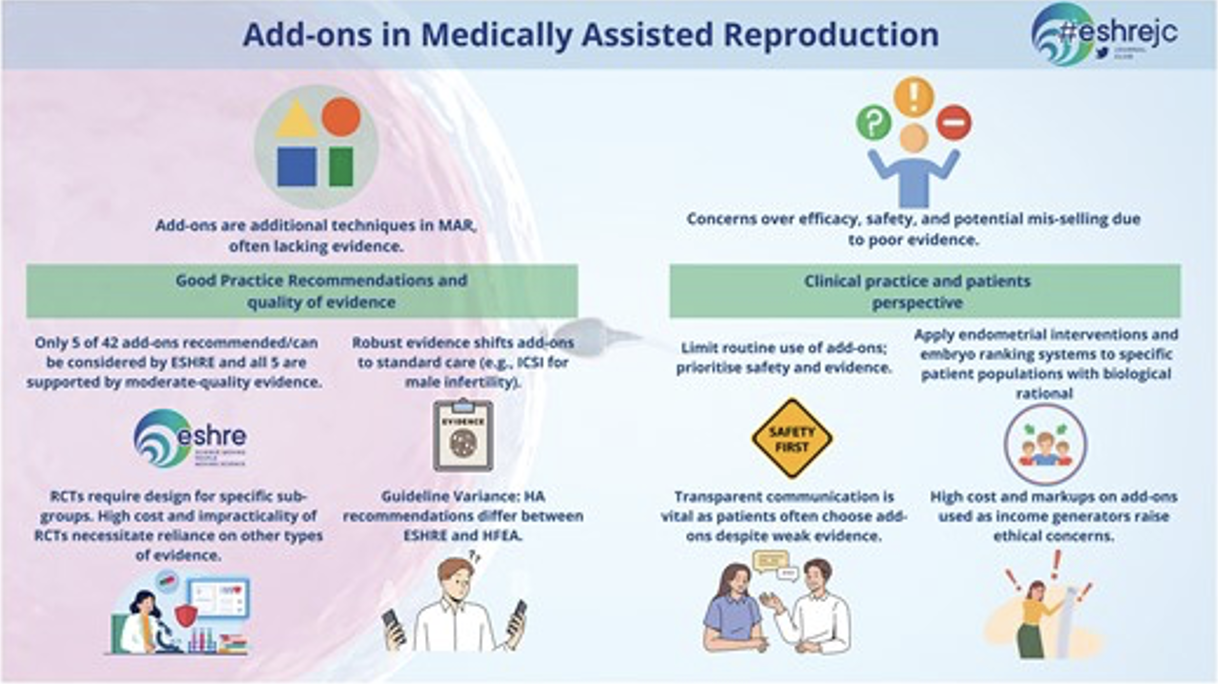
Figure 1. Graphic abstract of here discussed paper defining ESHRE’s approach to “add-ons” in reproductive medicine having led to not less than 42 recommendations covering diagnosis, diagnostic tests, laboratory tests in general, interventions, and clinical management.
Most importantly, however, many “add-ons” have potential for harm among those some immunological treatments with potential for significant side effects, which can introduce unnecessary medical risks without improving pregnancy and live birth rates (7). Misuse and/or overuse of PGT-A in younger patients may unnecessarily discard viable embryos, reducing a patient’s cumulative chances of success (8).
Having originally invented the term “add-on” to IVF to describe mostly unvalidated additions to routine IVF practice with the alleged intent of improving IVF outcomes, European colleagues have, of course, earned the right to do with this term whatever they wish. But, that also means that we can criticize what they have done with this term and, based on a recent publication in Human Reproduction by not fewer than 14 authors from all over Europe, apparently continue to do, as the graphical abstract of this paper above well documents (Figure 1) (9).
ESHRE’s effort, as described in above cited paper is, of course, laudable and exceeds in detail and quality everything offered by its counterpart in the U.S., the ASRM/SART conglomerate. But because it is so comprehensive and expansive, it also dilutes the message, - and that is a pity.
As the paper noted, the lack of regulation for the use of “add-ons” and the often very limited requirements for inclusion of “add-ons” into routine clinical IVF practice resulted in many cases in their introduction to market and routine clinical utilization without proper prior validation studies.
This fact is, in itself, indeed a good reason to develop evidence-based guidelines and information to help patients as well as physicians in making informed decisions about their use. But 42 such recommendations, consisting of four diagnoses and diagnostic tests, 17 laboratory tests and interventions, and 21 clinical management “add-ons” in our opinion are too much, and overwhelm patient as well as physician audiences. But even more importantly, they suggest that all 42 recommendations are equally important and that is, of course, very misleading.
ESHRE categorized the 42 “add-ons” it currently addresses in its good practice recommendations into four groups: (i) “recommended;” (ii) “can be considered;” (iii) “currently not recommended for routine use;” and (iv) “currently not recommended.” It is worthwhile noting that only 5/42 reviewed “add-ons,” ultimately, were “recommended” or described as “can be considered.” The remaining 37 “add-ons” were “not recommended for routine clinical use” or outright “not recommended.”
The CHR’s investigators already in 2019 identified preimplantation PGT-A as a very likely principal contributor to declining live birth rates in autologous IVF cycles around the world between 2010 and 2016 (10). A recent still unpublished study of the CHR then, in addition identified the explosive growth of all-freeze cycles in the U.S., mandating delayed frozen-thawed embryo transfer cycles in place of fresh embryo transfers, as the major culprit for the continuing linear decline of IVF cycle efficiency in producing live births until the year 2021 (Gleicher et al., unpublished data).
PGT-A and all-freeze IVF cycles replacing fresh embryo transfers, therefore, are likely the two practice changes in IVF most responsible - not only for IVF after 2010 having failed to further improve outcomes – but for the fact that live birth rates in the U.S., indeed, have declined by approximately one-third since 2010. Shouldn’t this fact alone earn these two practice changes, therefore, special attention from ESHRE (and for that matter also ASRM and SART, its U.S. counterpart)? We certainly think so!
Another excellent example for how illogical this list of 42 “add-ons” is, presents itself in the fact that only 1/42 of these “add-ons” was outright “recommended,” and that was – almost bizarrely – that high concentrations of hyaluronic acid (HA) in transfer media “may improve live birth rates in fresh embryo transfers.” Even assuming that really to be the case, that ESHRE giving this single “add-on” the only top grade, of course, says a lot about the other 41 reviewed “add-ons,” but also documents the absurdity of - intentionally or unintentionally – for all practical purposes equating all 42 listed “add-ons” in the mind of the IVF field by addressing them all together as if they had identical impacts on IVF practice.
What instead is needed is not the kind of bureaucratic ranking of these 42 “add-ons” offered by ESHRE, but a clear and statistically accurate assessment of how these 42 “add-ons” have been affecting IVF practice. Should such an analysis then, indeed, confirm the prominent adverse outcome effects of especially PGT-A and all-freeze cycle reported by the CHR’s investigators, then it appears high time for our professional organization to stop playing bureaucratic games by giving “add-ons” fancy designations without logical follow up, as – for example at the end of 2024 again happened, when the ASRM’s and SART’s ethics committees, years overdue, finally opined that PGT-A after over 20 years of increasing clinical utilization in general infertile patient populations still has no definable clinical utility and in certain sub-populations may actually reduce live birth chances (11).
Yet, after over 20 years of unbroken constant increases in PGT-A utilization, neither ASRM/SART nor ESHRE (or for that matter any other professional genetic society for example) has been able to reach the only logical next conclusion that, - if something has not improved outcomes in over 20 years of promised outcome improvements, isn’t it high time to stop using this treatment, especially when it – in addition – adds significant costs to an already exorbitantly expensive IVF cycle?
References
1. Perrotta M. Biomedical Innovation in Fertility Care. Bristol University Press. July 16. 2024; pp21-47
2. Maheshwari et al., Reprod Biomed Online 2016; 32(2):142-146
3. Idem. Hum Reprod 2022;37(3):476-487
4. Human Fertilisation & Embryology Authority (HFEA) 2023; Treatment add-ons. www.hfea.gov.uk
5. Lensen, S. et al. 2021. Cochrane Database of Systematic Reviews, Issue 6. Art. No.: CD009517. DOI: 10.1002/14651858.CD009517.pub4.
6. Harper et al. BioMedicine Online,2017; 34(6), 583-587.
7. Wheatley et al. J Reprod Immunol 2020; 137, 103078
8. ESHRE. Hum Reprod Update 2021; 27(1), 1–1
9. Serdarogullari et al., Hum Reprod. 2025, 40(2):398-404
10. Gleicher et al., Hum Reprod Open 2019(3):hoz017
11. ASRM Practice Committee Documents. The use of preimplantation genetic testing for aneuploidy ; A Committee Opinion (2024). https://www.asrm.org/practice-guidance/practice-committee-documents/the-use-of-preimplantation-genetic-testing-for-aneuploidy-a-committee-opinion-2024/