

General Gynecology, Menopause, & Sexual Medicine

Updates on endometriosis
Endometriosis & the immune system
A recent paper in Human Reproduction asked two important questions about endometriosis: (i) Are immunological diseases more frequent in patients with endometriosis? and (ii) in case this is, indeed, so, does a shared genetic basis contribute to the risk?
And the answer from a multi-center international group of investigators—unsurprisingly—was that endometriosis patients, indeed, demonstrate more autoimmune, auto-inflammatory, and mixed pattern diseases (a finding known for decades).1 But a GWAS analysis did offer new detail: Diseases with increased prevalence included rheumatoid arthritis, multiple sclerosis (MS), celiac diseases, osteoarthritis, and psoriasis, with genetic correlations between endometriosis and osteoarthritis, rheumatoid arthritis, and MS, and a potential even causal link to rheumatoid arthritis. The risk for developing a classical autoimmune disease was increased over controls by 30-80%. Endometriosis and osteoarthritis share 3 genetic loci, and rheumatoid arthritis shares 1 locus with endometriosis.
Interestingly, the paper referenced a publication by the CHR’s Medical Director and Chief Scientist, Norbert Gleicher, MD, in which he already in 1987 asked the question whether endometriosis was not an autoimmune disease.2
Endometriosis & pain
Somewhat related, another recent paper suggested that diet can reduce endometriotic pain.3 And, considering that endometriosis is now widely accepted as a neuroinflammatory disease, why should that not be (see figure below)?
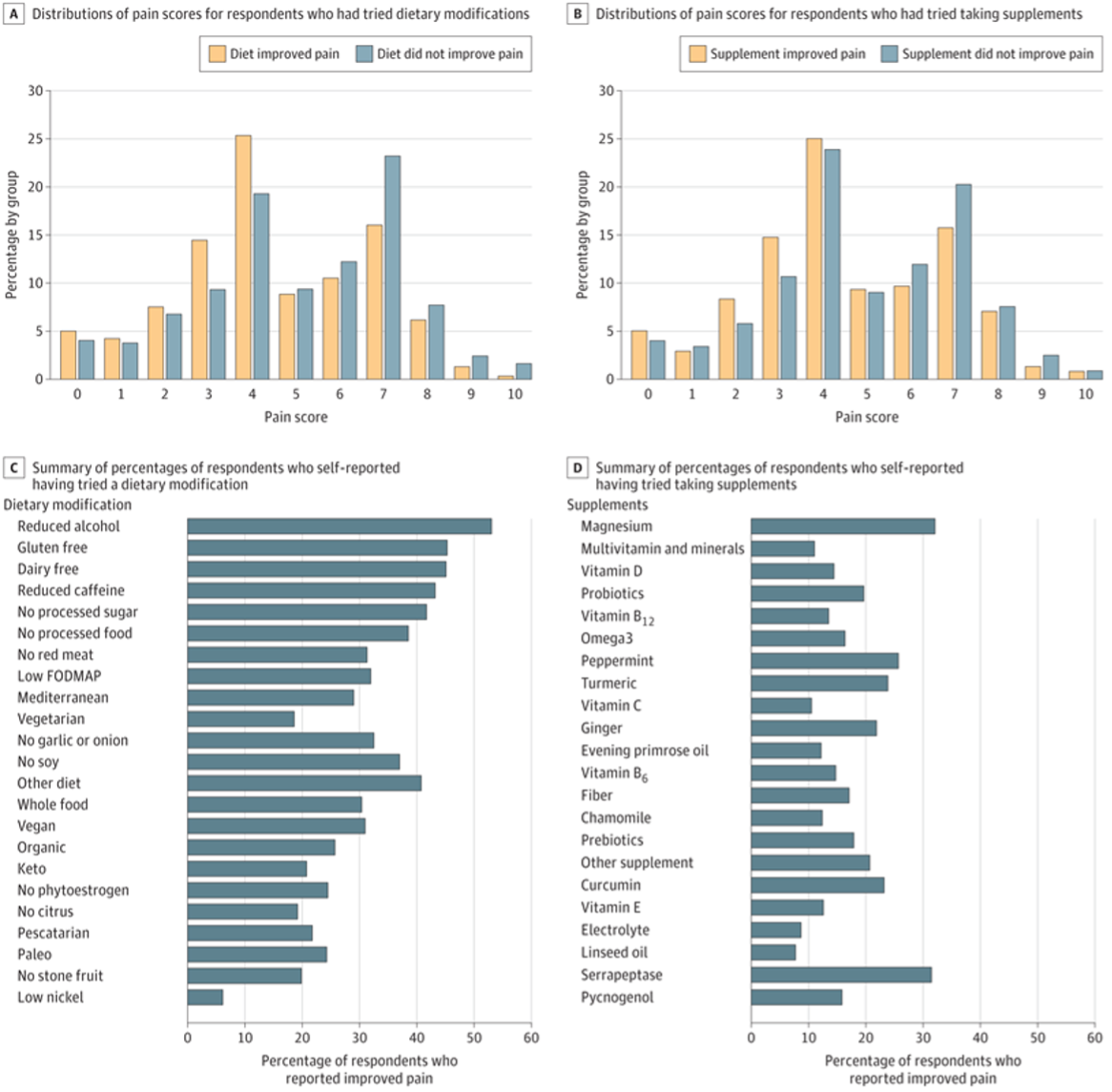
The above figure reports the number of survey respondents who reported using diets or supplements. It is difficult to make much detailed sense from this study (even aside of the fact that survey studies are notoriously unreliable); but there are nevertheless a few interesting observations to be made: For example that anti-inflammatory diets, reflected in no gluten and dairy intake, were the second and third most frequently taken steps is of interest and makes sense, though we must admit that the fact that alcohol was the most frequently excluded dietary component, was somewhat of a surprise.
Endometriosis & menopause
Another paper in the same journal asked yet another question, which to a large degree has already been answered: Is endometriosis associated with the type and age of menopause? And once again, the answer is not much of a surprise: Women with endometriosis showed a 7-fold increase in surgical menopause and were more likely to experience both natural as well as surgical menopause.4 In contrast to the previous study, we, however, did not learn much new information.
References
Shigesi et al., Hum Reprod 2025;40(6):1195-1209
Gleicher et al., Obstet Gynecol 1987;70:115-122
Heran-Yeates et al., JAMA Network Open 2025;8(3):e253152
Chung H-F, et al., Hum Reprod 2025;40(6):1210-1219
Updates on the Polycystic Ovary Syndrome (PCOS)
PCOS & the endometrium
If you were not aware that PCOS affects the endometrium, you are probably not alone, since this has not been a very prominent subject in the literature. But a recent paper in Nature Medicine kind of rekindled the interest in the subject with the publication of a single-cell atlas of the endometrium, since it demonstrated that PCOS alters the endometrium’s cell composition. The consequences are disruptions of hormone signaling and impaired receptor signaling, negatively affecting receptivity of the endometrium, increasing miscarriage risks, and also increasing the risk for endometrial cancer.1
PCOS patients were overweight and demonstrated obesity, hyperandrogenism, and insulin resistance compared with controls of similar age and, therefore, larger weight and body mass index (i.e., they apparently did not include lean phenotype-D patients under Rotterdam criteria in the study). Analysis of 5 control patients, 12 PCOS cases at baseline, and 7 after 16 weeks of Metformin treatment, and 3 after lifestyle intervention revealed cell-type-specific disease signatures and variations in cellular composition and localization. Samples taken after 16 weeks of Metformin treatment and lifestyle management showed extensive recovery from their disease-specific endometrial signatures.
The authors were also able to link specific roles of each cell type to clinical features such as hyperandrogenism and insulin resistance, and the risk of endometrial and metabolic disease. In addition, potential therapeutic targets such as integrin inhibitors were identified, and the role of Metformin in restoring endometrial health in patients with PCOS was highlighted.
This is an important paper since it informs on several new issues regarding PCOS: First, it reemphasizes the possible pathology caused by the condition in the endometrium, raising the question how to diagnose it and whether it exists in a given patient and, second, it raises therapeutic questions, as—for example—should all PCOS patients receive Metformin treatment?
Considering the damage PCOS-affected endometrial cells demonstrated in this study and how well Metformin remedied this damage, the answer may very well be a strong yes (of course, initially in the form of a clinical trial). But this is also the time to remember that this study did not include women with the lean PCOS phenotype (phenotype D) which differs from phenotypes A, B, and C in two typical ways: (i) it is not hyper-androgenic; and (ii) it is not associated with the metabolic syndrome at more advanced age but demonstrates a very strong association with evidence for a hyperactive immune systema and, therefore, with increased miscarriage risk.2 Metformin in these women, therefore, may not have the same beneficial effects.
PCOS and genetics
That PCOS is a polygenic inherited disease has, of course, been known for some time. Some candidate genes have, indeed, been described for obese and/or lean PCOS patients.3 The most potent variants were 4 unique variants in lean PCOS, 2 unique variants in obese PCOS, and 5 common variants in both. The study found that leptin signaling impairment and insulin resistance, as well as mutations in CYP1A1, CYP19A1, ESR1, AR, AMH, AdipoR1, NAMPT, NPY, PTEN, EGFR, and Akt, all played significant roles in PCOS.
In parallel, the literature also reflected a familial male pattern of PCOS.4 Now, however, a paper in the JCEM for the first time reported that brothers of PCOS patients demonstrate a higher risk for developing hypertension, obesity, and type 2 diabetes, in other words, of developing metabolic syndrome.5 Ever more evidence that the genetic background to PCOS in women also exists in males.
References
Erikkson et al., Nat Med 2025;31:1925-1938
Gleicher et al., Biomedicine 2022;10(7):1505
Dhar S, Bhattacharjee P. Sci Rep 2024;14:24468
Di Guardo et al., Int J Fertil Steril 2020;14(2):79-83
Kanina et al., J Clin Endocrinol Metab 2025; dgaf121, https://doi.org/10.1210/clinem/dgaf121
Update on menopause—use it or lose it
Japanese investigators published an interesting paper in Menopause, investigating the association between regular sexual activity and sexual function of women in menopause and the so-called genitourinary syndrome-related symptoms. And—can we say unsurprisingly—the study demonstrated an association between regular sexual activity and low prevalence of symptoms relating to the syndrome. In other words, “use it or lose it” applies here as well!
Reference
Yoshikazu et al., Menopause 2025;32(7):592-600