

GENERAL NEWS FROM THE FERTILITY FIELD

Today’s posting offers a broad spectrum of news for almost everybody in one or the other way engaged with the fertility field. We are addressing change in the pharma industry which over decades has failed to innovate when it comes to either female or male infertility. Diagnostics – we must say – have also not been too hot and, indeed, o several occasions have succeeded bringing to market pretty useless stuff. But there can be no doubt that change in the fertility field in general has been speeding up and we are with today’s posting attempting to offer a quick overview.
We hope you enjoy today’s postings and, as always, are looking forward to your responses.
The CHR’s Editorial Staff

News from the Fertility Pharma Industry
The Inside Reproductive Health (IRH) , made several interesting points in a recent report worthwhile mentioning here:1
Disruptions at drug manufacturers like big layoffs at Ferring and the exit of the Organon CEO , Kevin Ali, – for at least so-far – appear not to have impacted the companies’ fertility operations (yet). But Ali’s exit from Organon, of course, appears related to the since announced pending acquisition of Organon by India’s Sun Pharma in an $ 11.75 billion all cash deal.1 Serono’s early announcement about quite radical price reductions for their company’s gonadotropins in response to the Trump administration’s effort to lower medication pricing will, however, of course force the hand of competitors. Amazing how large the companies’ profit margins on these medications must have been if Serono could afford such big discounts!
Even more interesting, the report correctly noted that new drug R&D in the fertility arena has – to say it politely - dragged for decades. More bluntly, it basically has not existed with the reason being that, previously independent pharma companies almost exclusively active in the fertility field, were bought up by multispecialty giants who quickly discovered how small the fertility market really was in comparison to many other medical specialty areas. Investments toward the developments of new drugs, therefore, went elsewhere.
The article in IRH now suggested that, driven by newer companies in the field, this decades-long drought may now have finally ended. One such company is Granata Bio which apparently partnered with Gedeon Richter, - a very prominent European pharma company to bring an additional FSH to the U.S. market after – because of the staggering costs of FDA approvals - so-far having chosen not to enter the U.S market. These two partners also acquired Oviva Therapeutics, - a relatively new company concentrating on the ovarian aging process, finally including production of a hypoglycosilated FSH products, fitting natural glycosylating changes observed in the FSH of aging women.
The CHR’s Medical Director and Chief Scientist, Norbert Gleicher, MD, - and we are certain others – suggested such adjustments – to no avail - in FSH glycosylation based on patient ages to the old-timer companies in the fertility field, Serono, Organon, and Ferring already decades ago. Their response was negative because they argued that this would only split the already existing (relatively small) market.
A company called Meitheal, in turn, has taken the lead in bringing generic fertility medications to market in the U.S (Genirelix and Cetrorelix) and is also advancing a FSH biosimilar.2
News About Fertility Diagnostics
A recent posting suggested that payor preferences as well as clinical workloads bring at-home testing to the forefront, with home semen analysis being a good example.3 The big home-testing reward for patients as well as IVF clinics would however, of course, come from the ability to monitor patients in ovarian stimulation cycles from home.
Pulsenmore, the Israeli ultrasound manufacturer that already received FDA approval for home pregnancy monitoring,4 in January now also announced home follicle size monitoring.5 But follicle size alone is, of course, not enough to determine ovulation trigger timing. For that, additional blood tests are required (estradiol, progesterone and sometimes LH). That is, - they were required:
The CHR’s investigators, indeed, recently filed a patent, describing a technique that allows assessments of follicle maturity (and, therefore, egg maturity) by using only ultrasound alone. If validated by further studies, this new patent will, indeed, allow home monitoring of patients in all ovarian stimulation cycles, including IVF cycles. Imagine what difference that would make for patients as well as IVF clinics!
News About Third-party Donations
As another report by IRH noted,6 the use of third-party donations in the U.S. appears “strained.” And the strain is apparently at least partially the consequence of increasing demand. The CHR fully agrees that many third-party programs including gestational carriers, surrogacy agencies, sperm banks, and egg banks -as the report noted - “simply don’t meet the operational standards required to seamlessly support the patient experience.” We have noticed especially increasing inconsistencies in donor egg quality and especially in the selection process for gestational carriers, while costs for these services are continuing to increase. In other words, patients are asked to pay more for less!
The Adoption of A.I. by Fertility Clinics
Yet another IRH report suggested that during 2025 the adoption of A.I. in fertility clinics accelerated.7 But that is, of course a very relative term. Our impression, indeed, is that A.I. – as of this moment of time – in infertility plays a much smaller role than in some other medical specialty areas. While that may change, we know of at least one A.I. start-up that – after a lot of initial publicity - already went out of business. It originally claimed outcome advantages for IVF from judging embryo development by A.I. through imaging systems. Advantages of its algorithm apparently were not worth time and financial investments.
In a retrospective cohort study of 858 patients, a company called Cycle Clarity apparently found that A.I.-only follicular ultrasound produced outcomes equivalence to traditional monitoring using ultrasound and hormone levels. Its website describes it as follows: Cycle Clarity is software company dedicated to improving fertility care around the world. It’s FDA-cleared patented software platform can reduce fertility ultrasound times from 15 minutes to 20 seconds while simultaneously adding standardization of follicular measurements and providing clinical decision support software to enhance decision making.
Every time in recent years when a new “add-on” to IVF was announce as “time-saving” we so-far have been disappointed and, therefore have become quite skeptical - but are looking forward to more information. Every IVF clinic these days would benefit from time savings!
Declining Reimbursements for IVF Clinics
Declining reimbursement rates have apparently been “slashing fertility centers’ margins.” Employer benefit managers and insurance companies per this report often reimburse fertility clinics only at a fraction of only around 50%.8
Ever poorer insurance reimbursements are, of course, nothing new, - leading the CHR already over 20 years ago to limit the insurance plans CHR was willing to accept to plans that at least covered CHR’s overhead costs per cycle. A 50% reimbursement rate form regular fee schedules very definitely doesn’t do that. In most clinics, but certainly in those which basically accept any insurance plan, cash-paying patients – without even knowing - thus subsidize insurance covered patients.
The State of the Fertility Clinic Networks
In a quarterly review IRH also summarized how fertility clinic networks, mostly owned by Private Equity, are expected to perform in 2026,9 - and the conclusions were not very pretty and we are quoting: (i) “Everyone is freaking out” because of fierce competition for fertility specialists.” (ii) We are already witnessing a backlash against these practice networks.
And what are the signs? A first one is that most of them are looking for buyers, including US Fertility where Amulet Capital partners was unable to sell their majority ownership and only succeeded to decrease its exposure by bringing in L. Chatterton which acquired a 42.5% stake in the company. Management and the roughly 200 physicians the company employs, thus are left with only 15% ownership. Other networks are allegedly behind the scenes – so far unsuccessfully - searching for buyers are, - Kindbody already for over a year, Inception, Pinnacle, and others also for some time.
A second reason is that individual REIs and/or small groups of physicians are returning to opening their own “little” practices. So, for example – as we previously already reported in the CHRVOICE, three REIs from Boston IVF opened their own practice at home in straight competition to Boston IVF in Boston.
REFERENCES
Venkat PR, Loftus P. The Wall Street Journal. April 22, 2026. https://www.wsj.com/business/deals/sun-pharmaceutical-to-acquire-organon-valued-at-11-75-billion-8c3e0f65
Inside Reproductive Health. January 15, 2026, https://www.linkedin.com/pulse/state-fertility-pharmacies-2026-insidereproductivehealth-jpfac/
Inside Reproductive Health, January 13, 2026, https://www.fertilitybridge.com/news-articles/fertility-diagnostics-at-home-testing-2026
Radiology Business. November 3, 2025. https://femtechinsider.com/pulsenmore-and-clalit-health-services-launch-at-home-follicular-monitoring-for-ivf/
Israel.com. January 27, 2026. https://israel.com/technology/pulsenmore-clalit-launch-israels-first-at-home-fertility-monitoring-service/
Inside Reproductive Health, January 15, 2026. https://www.fertilitybridge.com/news-articles/third-party-ivf-patient-experience-breakdown
Inside Reproductive Health, January 13, 2026. https://www.fertilitybridge.com/news-articles/artificial-intelligence-fertility-care-2026
Inside Reproductive Health ,January 14, 2026. https://www.fertilitybridge.com/news-articles/ivf-benefits-patient-finance-2026
Where the Infertility Field Is in Attempts to Favorably Influence the Ovarian Aging Process
We have – especially in recent times – been quite critical about what Fertility and Sterility - in the format of opinion articles (which, of course includes many different review formats) has been publishing. We, therefore, were in a way positively surprised to see in the March 2026 issue of the journal and interesting and somewhat original View and Review article (this designation correctly described the article) that informed well on ongoing attempts to learn how to potentially influence to the better ovarian aging.
The article format was “original” because the paper had five distinguished authors from different institutions who apparently – separately - wrote five individual sections of the manuscript: (i) An introduction (2 authors); (ii) clinical applications and experimental modalities including platelet-rich plasma, stem cell therapy, and mitochondrial transfer (2 authors); (iii) nutrient-sensing pathways, including the growth hormone - IGF-1 and rapamycin (mTOR) pathways (1 author); (iv) partial epigenetic reprogramming and ovarian aging, including methylation, histone modifications, and chromatin organization (1 author); and (v) ovarian fibrosis as target for reproductive longevity (also discussed earlier in this section, - 1 author).
All five sections are very well written, objective, and well referenced, - a review article that not only informs but also educates.
REFERENCE
Eubanks et al., Fertil Steril 2026;125(3):387-398
Does Anybody in Fertility and Sterility’s Editorial Office Peer Review the Journal’s “Inkling” Articles?
This is, of course, not the first time – and with great likelihood also not the last time - that we criticize an “Inklings” article in Fertility and Sterility.
There are many, we think good reasons, why we don’t like “Inklings: (i) Based on the Merriam – Webster Dictionary, it’s a really stupid name since this noun reflects “a slight knowledge or vague notion,”1 - certainly not what readers of F&S would expect from an allegedly authoritative editorial which is only open to submissions from the journal’s unusually large editorial board. (ii) While opinion papers may be good for improving the various citation indices of a journal, they, of course lower the scientific appreciation of the journal, especially if their publication, like in the case of F&S, greatly reduces page numbers dedicated to scientific papers. After all, expert opinion represents the lowest level of evidence in the evidence pyramid. Every kind of study, therefore, represents better evidence than an Inkling. (iii) But definitely the most compelling reason is their - only too often – not very informative content that makes one at times wonder whether Inklings are subject to even minimal peer review or – after submitted by a member of the editorial board - are automatically allowed into print.
The March 2026 issue of F&S offered again a telling example when three authors (under the obvious leadership of a senior editor of F&S who in recent years contributed opinion articles on all kinds of subjects to almost every monthly issue of the journal), practically issued an order to the troops (sorry, - we meant readers) categorically demanding to “not measure antiMüllerian hormone to predict women’s fecundity (this is how the hormone was, indeed, spelled)!”2
To further explain why this Inkling article warranted our commentary, we here verbatim cite its concluding paragraph (in its at times stylistic awkwardness):
“The routine measurement of AMH in young women for counseling them about their fecundity is fundamentally flawed. This practice, still too often and undertaken, may lead to unnecessary and unfounded fears in women whose AMH is low. Reproductive doctors (we assume that is us) and women alike should know that routine AMH dosage (??? - we assume what was meant was level or concentration) for fertility counseling provides false information and should be absolutely discouraged. Let this be a call to action (Liberté, Égalité, Fraternité???) to raise awareness within both the public and the obstetrics and gynecology communities about the limitations of AMH testing and to end the misguided practice.”
So, what are these authors really telling us with their Inkling article?
It sure sounds like we should stop measuring AMH levels in our female infertile patients. And why? Because – and we are quoting again verbatim from the article: Already “over 18 years ago, we (the meaning is only the senior author of the Inkling article) first reported live pregnancies in women whose AMH levels were undetectable and had been advised to undergo donor-egg ART (and, of course referencing themselves in a 2008 F&S publication3). The Inkling article then went on to another paper – of course again of the senior author - noting that “over 10 years ago” it reported “expected age-related decreases in AMH after (prolonged) oral contraceptive use and that time to subsequent spontaneous pregnancy was unrelated to their measure of AMH levels.”4
The Inkling article then cited two additional later published papers by different authors, claiming that AMH levels are unrelated to natural conception.,5,6 - which the Inkling paper then used in support of its professional tongue lashing of us reproductive doctors for still using AMH levels for screening purposes.
And aside of the fact that medical journals (other than seemingly F&S, of course) have started to notice and address during peer review excessive self-citations, the Inkling’s argument does not make logical sense because nobody with basic understanding of AMH functions will use AMH levels exclusively to predict the future fecundity of a patient (if we at the CHR did this, we would have no patients considering how low even our younger patients’ AMH levels are). But that does not mean that women, in whom either a problem with functional ovarian reserve is already suspected or because their medical history may suggest an increased risk for premature ovarian aging (POA), should not be screened with AMH.
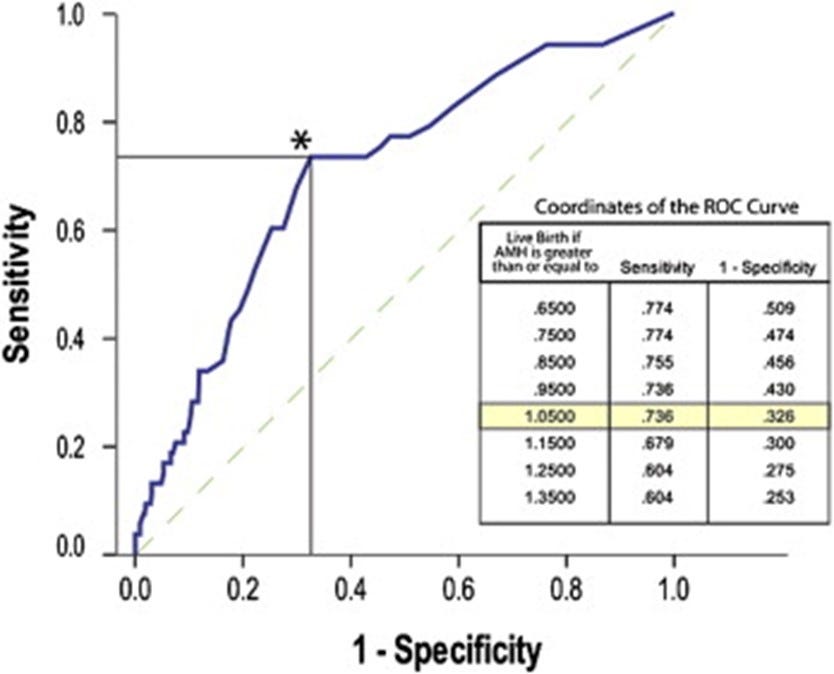
Let us here – coincidentally - quote from an F&S paper by CHR investigators published already in 2010 (and, of course, unreferenced in the Inkling article) under the title, - “Anti-Müllerian hormone (AMH) defines, independent of age, low versus good live-birth chances in women with severely diminished ovarian reserve.”7 And we quote from the abstract of this publication:
“Maximal receiver operating characteristic curve inflections, which differentiate between better and
poorer delivery chances in women with diminished ovarian reserve (DOR) independent of age, were at anti-Müllerian hormone (AMH) 1.05 ng/mL (improved odds for live birth 4.6 [2.3–9.1), 95% confidence interval: Wald 18.8, df = 1], although live births occurred even with undetectable AMH. Pregnancy wastage was very low at AMH ≤0.04 ng/mL but significantly increased at AMH 0.41–1.05 ng/mL, resulting in similarly low live-birth rates at all AMH levels ≤1.05 ng/mL and significantly improved live-birth rates at AMH ≥1.06 ng/mL (see figure below).”
So, why then does “do not measure antimüllerian hormone to predict women’s fecundity” not make any sense (beyond the strange spelling)? Because AMH – besides reflecting functional ovarian reserve (i.e., potential egg numbers in an IVF cycle) – also reflects other hormonal influences (i.e., for example hormonal contraceptives). And anybody who is aware of these associations, consequently, will not be stupid enough to refer a young women automatically into egg donation because she had a very low AMH level or may not even demonstrate any detectable AMH at a given moment.
AMH is, therefore, quite good in predicting response to stimulation but far less good in predicting pregnancy chances in IVF (especially in the longer run), But because egg and, therefore, embryo numbers are predictive of cumulative pregnancy chances (of course, also taking age and other factors into account), AMH also has relevance in predicting pregnancy chances but, of course, to lesser degrees. To basically state that AMH should not be tested to predict a woman’s fecundity, therefore, is simplistic thinking, - undeserving of an editorial opinion in a leading fertility journal.
REFERENCES
Merriam – Webster. https://www.merriam-webster.com/dictionary/inkling. Accessed March 17, 2026.
De Ziegler et al. Fertil Steril 2026;125(3)399-400
Fraisse et al., Fertil Steril 2008;89:723:39-11
Streuli et al., Fertil Steril 2014;28:216-224
Zarek et al., J Clin Endocrinol Metab 2015;100:4215-4221
Galati et al., Arch Gynecol Obstet 2024;310:2691-2696
Gleicher et al., Fertil Steril 2010;94(7):2824