

Making IVF Always More Expensive, But - Unfortunately - Never any Better in Outcomes!

Today’s posting involves an Editorial by the CHR’s Editorial Board and, therefore, represents the opinion of the CHR and clinical as well as ethical practice principles of the CHR. For that reason, we reserve this publication format to only include the most important issues that arise in the fertility field.
The CHR has for many years been on record as a leading opponent of several so-called “add-ons” to IVF. CHR investigators have pointed out in several papers over almost 20 years that these add-ons have not only failed patients in improving IVF outcomes, but also in many instances have actually harmed IVF cycle outcomes in selected patient populations. They, of course, uniformly also significantly increase IVF costs.
Examples abound,- from preimplantation genetic testing for aneuploidy (PGT-A), polygenic risk screening of embryos (PGT-P), routine all-freeze cycles with delayed frozen embryo transfer cycles, - to many more. The CHR in many of these publications has also criticized the frequently observed silence of professional societies in the fertility field in this matter.
Today’s Editorial was spawned by an article by several prominent European colleagues who claimed that the poor IVF outcomes in poor-prognosis patients should be “fought” not with better cycle management (maybe excluding some of the above-noted harmful “add-ons” to IVF in such patients), but by simply manipulating outcome data, - so they looked better by no longer presenting outcomes to patients based on single-cycle outcomes, but based on multiple-cycle outcomes. In other words, - sell IVF to poor-prognosis patients in multiple-cycle packages (which, of course, lock patients into multiple-cycle commitments). One, therefore, wonders who would really benefit from this kind of a change? Certainly not the patient!
The CHR’s Editorial Staff

Making IVF Always More Expensive, But - Unfortunately - Never any Better in Outcomes!
The Editorial Board of the CHRVOICE and The Reproductive Times
Sometimes it is not enough to speak quietly, and raising one’s voice becomes essential if one wants to be heard at all. In this article, the CHR’s Editorial Board does exactly that when addressing the fact that the IVF field is overrun by a stampede of great-sounding clinical ideas, - including so-called “add-ons”- offered by often prominent “experts” in the field and introduced into routine clinical practice, - simply based on the power of the names of the “experts.” And as is well recognized, expert opinion – yet deservedly - sits at the very bottom of the evidence pyramid because a good idea is, of course, cheap and not at all enough to support introducing new treatments, - even if such treatments – especially if not depending on FDA approval - at times can also become quite profitable.
Colleagues often too generously offer such opinions through the quickly increasing plethora of opinion articles in many medical journals, sometimes with clear intent, - but frequently simply out of ignorance about potential negative consequences.
This Editorial was in reaction to such a recent article in a prominent European infertility journal, which – without any cost and other considerations like time to pregnancy - claimed to introduce a new treatment paradigm with the goal of benefitting clinical patient outcomes. Though patient outcomes, of course, must be at the center of all benefit considerations, they also must not exclude risk assessments and costs. Both of these considerations, however, did not at all enter consideration in this proposal, and that must be viewed by editors as a clear warning signal before publication that other than pure scientific considerations may be - subconsciously or consciously - at the core of a new submission for publication.
We fully recognize the controversial nature of this Editorial, but, considering the uncontrolled proliferation of unvalidated “add-ons” to IVF practice since approximately 2010, the IVF field will not improve IVF cycle outcomes that have stagnated since that date overall, and for certain patient sub-groupings (like autologous IVF cycles), they have actually dramatically declined. Because of the controversial nature of this Editorial, we – more than ever – are looking forward to our readers’ opinions.
Especially our European colleagues always appear on the outlook for new ideas about IVF, - but for some reason, - those ideas never appear to improve IVF outcomes as promised. They most certainly, however, increase IVF costs. And, paradoxically, it almost appears like, – the more expensive, the quicker the new ideas are accepted by the IVF field, - even in absence of significant evidence. There is, of course, reason to wonder why this has been such a recurring theme?
When Austrian/German colleague Georg Griesinger, MD,1 for the first time in 2007, and Paul Devroey, MD and colleagues in Brussels, Belgium2 in 2011, for example, proposed so-called segmentation of IVF, a term created to denote the conceptual separation of ovarian stimulation from embryo transfer, the primary purpose was to prevent the ovarian hyperstimulation syndrome (OHSS) in IVF cycles with excessive follicle numbers. The idea of all-freeze cycles under such circumstances, then, of course, made sense.
But what followed was that the concept then was expanded to practically all IVF cycles under the dubious – and, to this day, unproven – allegations that ovarian stimulation in IVF cycles in some ways adversely affects endometrial receptivity. And, suddenly, all-freeze cycles became the “fashion of the moment” (and, yes, IVF constantly does go through such “fashions of the moment”) for all IVF cycles after they were heavily promoted by Las Vegas-based Bruce S. Shapiro, MD, and co-workers (too much gambling going on in Las Vegas, apparently!).3 But that fashion did not maintain popularity because some “real” studies very quickly demonstrated that this kind of segmentation did not – as claimed by Shapiro et al (and others) – improve IVF outcomes, but actually reduced cumulative pregnancy chances.4 But by adding freezing costs and additional costs for a thaw-out frozen embryo cycle, it surely raised overall IVF costs (and, of course, increased IVF clinic income) significantly, while in addition prolonging the time to pregnancy.
But that is only one “fashion of the moment” that has obviously negatively affected IVF practice (and is still going on in too many U.S. and European IVF clinics). Again, especially some European colleagues have apparently convinced themselves that they know what we should spend our money on: A.I., of course, can improve donor oocyte assessment5 and basically everything else in embryology, DuoStim is, of course, effective in improving egg numbers (and how about quality?).6 It also, of course, prevents all fresh embryo transfers and, therefore, requires an additional thaw cycle; but who cares about that?
And, yes, all embryology, of course, must be automated7 (because closed incubation systems really delivered on all the promised improvements the manufacturers touted) and, therefore, let’s just expand automatization to everything in the embryology laboratory (and it, of course, helps if we hold shares in a company that sells the needed equipment).
A group of prominent European colleagues recently published a commentary in Reproductive Biomedicine Online (RBMO), in which they – kind of unexpectedly – proposed to “change the narrative for poor-prognosis patients in IVF by unlocking success through a multi-cycle approach.”8
So, why were we interested in this subject? Not only because one of the authors was a senior associate editor of the journal (the topic of editors publishing in their own journals was recently addressed in a prior issue of the CHRVOICE). No, - what we found, rather shamefully, was that these authors were not trying to suggest that it was time to try to improve the kind of IVF that is offered to poor-prognosis patients all over the world, - but they were suggesting the amazing – almost mind-blowing – allegedly new concept of offering them multiple-cycle packages as the solution for the patients’ poor prognosis.8 Not a word, however, on the fact that relatively promising treatments exist for many women above ages 42-43 that - even with autologous oocytes - still offer very decent pregnancy chances.
Most U.S. IVF clinics, however, are no longer even interested in trying to treat patients with their own autologous eggs. U.S. statistics well demonstrate this fact through the quick fall into nothing of U.S. autologous IVF cycles after age 43. This is indeed why we started this commentary with the subject of “all-freeze cycles.”
The authors, then, of course, also had to add to their absolutely “brilliant” idea of multiple-cycle packages in poor-prognosis IVF patients the following, -quoting the authors verbatim: “A multicycle approach, adopting approaches such as oocyte/embryo accumulation from several stimulations or two consecutive stimulations, - i.e., DuoStim (yes, they threw that in as well!), enables the advance planning of multiple attempts (really?). It helps shorten time to pregnancy (evidence?), reduces treatment discontinuation (evidence?), and offers support for patients facing setbacks (how?).
Poor-prognosis patients, of course, have poorer pregnancy chances than average-prognosis and especially good-prognosis patients. And, as usually one of the best-informed patient populations in all of medicine, infertility patients, of course, understand that – in practical terms – this means that they can expect to need more IVF cycles than most other patients. Multiple-cycle packages in such cases then, of course, may make sense for some patients, but, of course, only if significantly discounted.
But to make this the centerpiece of a Commentary article in a major infertility journal with not a word about how poorly poor-prognosis patients are currently treated (if at all!) in most IVF clinics is just further evidence for how much more emphasis is dedicated these days to improving the economics of IVF (for providers) rather than the execution of high-quality infertility care (for patients).
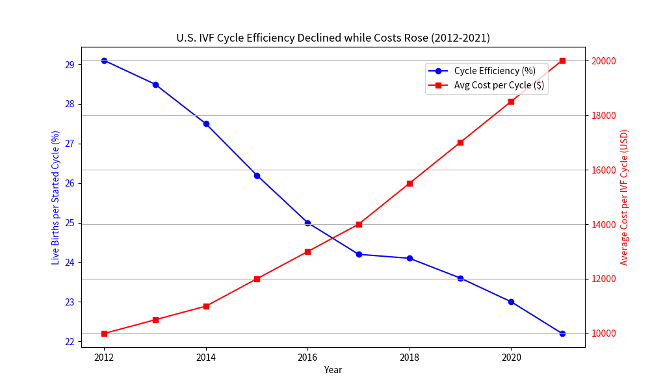
All of this must also be seen against the overall clinical realities of steadily declining pregnancy and live birth rates in autologous IVF cycles versus steeply increasing IVF cycle costs based on U.S. registry data (see figure below). Considering, under these circumstances, multi-cycle programs as the solution , - rather than advocating for better per-cycle outcomes first, appears more than just a misdirection. Since the “add-on” revolution around 2010 started to explode, these kinds of unfortunately only poorly-thought-through commentaries have, however, been fairly typical, - not infrequently driven by false narratives by European colleagues.
And the consequence?
To the best of our knowledge, autologous IVF - at least in the U.S. - has earned the “honor” of being the only widely accepted primary treatment in all of medicine which over the last 15 years has experienced an almost straight line downwards to progressively poorer outcomes (see again figure below, with background information for this figure provided as a footnote).
Three U.S colleagues recently submitted a letter-to-the-editor to Human Reproduction Open in which – describing themselves as “leaders of the Society for Assisted Reproductive Technology (SART),” a sister society of the American Society for Reproductive Medicine (ASRM) – they criticized a recently published paper in this prominent journal by CHR investigators that pointed out “the declining efficiency since approximately 2010 of (autologous) IVF in the U.S.,”9 as also described in the above figure. We, of course, are not permitted to reveal the content of their criticism before publication of their letter and the CHR authors’ response. But it appears appropriate to point out here that this Editorial made its points appear even more timely in view of the comments made by SART leadership in this letter and we strongly encourage the readers of this Editorial to seek out this exchange of letters, which should appear within weeks in Human Reproduction Open.
REFERENCES
Griesinger et al., Hum Reprod 2007;22(5):1348-1352
Devroey, et al., Hum Reprod 2011;26(10):2593-2597
Shapiro et al., Fertil Steril 2014;102;3-9
Wong et al., Hum Reprod 2021;36(4):998-1006
Cimadomo et al., Hum Reprod 2025;40(10):1886-1892
Vaiarelli et al., Upsale J Med Sci. 2020;125(2):121-130
Racowsky et al., Fertil Steril 2026;125(1):2-12
Vaiarelli et al., Reprod Biomed Online 2026;52(5):105465
Gleicher et al., Hum Reprod Open 2026(1):,hoag004